
M4 entry wound

M4 exit wound
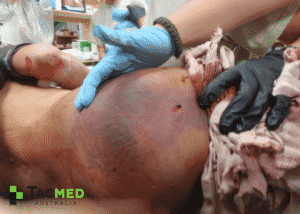
The preceding series of photos shows a particularly nasty M4 gunshot wound, with a small entrance wound in the right lower buttock, and a massive exit wound in the right lateral thigh. The X-ray in the last image shows that the projectile has struck the upper femur and demolished the bone, sending secondary bone fragments flying through the tissues and accounting for the magnitude of the exit wound.
The damage done by the pressure wave of the temporary cavity can be appreciated in the first image with deep bruising extending up the buttock and into the casualty’s lower back from the energy dissipated through the tissues pulverising small blood vessels in its path (think back to the ballistic gelatin video to imagine what went on in the tissues). The granular material in the middle of the thigh wound and seen on the X-ray is an older generation Quikclot Advanced Clotting Sponge (ACS) which was inserted at the point of injury for haemorrhage control, with excellent effect. The bright white fragments on the X-ray are small pieces of the bullet, which had disintegrated on impact with the tissue and bone.
This is another characteristic of the M4 round which makes it all the more unappealing to be shot with, that being the tendency for the bullet to disintegrate if it strikes tissue at a decent velocity. Despite being a jacketed round, owing to it being smaller, lighter, and faster than an AK47 projectile, it tends to yaw faster once it hits tissue, and the shearing forces on the bullet once it is traveling at 90 degrees through the tissue often tears the bullet into pieces, thus creating multiple smaller projectiles and increasing the chances of all of the bullet parts remaining in the target, and hence dissipating more energy.
The AK47 round, being slightly heavier and slower than the M4 round will have a tendency to remain intact as it strikes tissue, and whilst it will penetrate deeper, it tends to remain intact and not yaw until it has penetrated much deeper than the M4.
Here’s an example of the AK47 calibre 7.62x39mm being fired into ballistic gelatin for comparison to the video above of the 5.56x45mm (M4) round. Whilst the video shows a soft point round being used, which theoretically should be more destructive than its full metal jacket counterpart, the video still illustrates nicely the significant penetration of the AK47 round without it yawing significantly or disintegrating.
I once saw a good case study illustrating this point nicely where a casualty had sustained an AK47 gunshot wound to the right lateral thigh and we recovered the intact bullet from the inside of his left upper abdominal wall. It had passed through approximately 1 metre of his tissues and shredded his small bowel, but the projectile hadn’t fragmented at all, and the temporary cavitation hadn’t done enough damage to be lethal. The casualty required a laparotomy to remove multiple sections of small intestine but made a good recovery. That one is a story for another time.
The next photo is of a good friend of mine who was shot by an AK47 from approximately 200 metres whilst standing right next to me! Fortunately, the bullet passed cleanly through and after a surgical clean-out on the afternoon of the injury, he turned up ready for work the very next day. They breed them tough where he is from!

This image was taken a few days after the injury and the bruising from the temporary cavity of the projectile can be seen along the path of the bullet. The entrance wound is at the top of the left buttock, with the exit being down on the left upper thigh.
Although an unpleasant injury to have, the fact that the AK47 round was traveling slower than an M4 at the same range would have been, coupled with the fact that the projectile remained intact and didn’t yaw significantly as in passed through him, meant the wound was nowhere near as devastating as the above-mentioned M4 injury in the same area. It must be noted however that the comparison is far from perfect given that the M4 injury involved the bone, with the one immediately above passing solely through soft tissues.
So there it is, all things being equal, when all is said and done I’d rather be shot with an AK47 than an M4 on any day of the week. Naturally, as medical responders, it is always important to treat the wound and not the rifle that inflicted it, and I have certainly seen some horrendous AK47 wounds over the years and some relatively minor ones from M4s, it all depends.
The main take-home points for medicos are to be aware of the magnitude of damage that can be caused by the temporary cavitation resulting from high-velocity missile wounds, and also if you find an entrance wound, there’s no telling where in the body the projectile might have ended up!
Thanks for reading, comments and questions are welcome. Cheers, Dan Pronk.
If you enjoyed the article and feel that others in your network might also, please consider sharing.
_________________________
This article first appeared in The Havok Journal on July 22, 2018.

Buy Me A Coffee
The Havok Journal seeks to serve as a voice of the Veteran and First Responder communities through a focus on current affairs and articles of interest to the public in general, and the veteran community in particular. We strive to offer timely, current, and informative content, with the occasional piece focused on entertainment. We are continually expanding and striving to improve the readers’ experience.
© 2026 The Havok Journal
The Havok Journal welcomes re-posting of our original content as long as it is done in compliance with our Terms of Use.


